Arkansas Medicaid Prior Authorization Form
Arkansas Medicaid Prior Authorization Form - Web up to $40 cash back arkansas medicaid prior authorization form is not the form you're looking for? Information about where to get a supply of the forms and links to samples of. Service must be performed before the end of the. Search for another form here. To become a participating provider with empower, please complete the. Save or instantly send your ready. Web watch for your renewal form, fill it out, and return it to arkansas medicaid right away to avoid losing medicaid coverage if you are eligible. Web send completed form to: Web what can you do in the provider portal. Easily fill out pdf blank, edit, and sign them.
Web up to $40 cash back arkansas medicaid prior authorization form is not the form you're looking for? To become a participating provider with empower, please complete the. Navigate aba prior authorization form; Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request page 1 of 1 after completing the information below please fax to. Search for another form here. Arkansas foundation for medical care, inc., (afmc) – attn: Web prior authorization control number: Acthar gel (corticotropin injection) prior authorization (pa) request form. Web arkansas medicaid prior authorization forms | covermymeds manage your arkansas medicaid prior authorization requests our electronic prior authorization (epa). Web send completed form to:
Web to become an arkansas medicaid provider, please visit ar medicaid provider enrollment by clicking here. Search for another form here. Navigate aba prior authorization form; If an authorization is needed, you can access our login to submit online. Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request fax form to: Web watch for your renewal form, fill it out, and return it to arkansas medicaid right away to avoid losing medicaid coverage if you are eligible. Through this secure and easy to use internet portal, healthcare providers can submit claims and inquire on the status of their claims, inquire. Web send completed form to: Information about where to get a supply of the forms and links to samples of. Web up to $40 cash back arkansas medicaid prior authorization form is not the form you're looking for?

Free Arkansas Medicaid Prior (Rx) Authorization Form PDF eForms
Web send completed form to: If an authorization is needed, you can access our login to submit online. Web to prior authorize services for recipients under age 21, send completed pages 1 through 6 to: Web arkansas medicaid state supplemental rebate contract template.pdf may 26, 2023 4:17:32 pm certified behavioral health agencies (bha).pdf may 26, 2023 4:32:09 pm. Navigate aba.

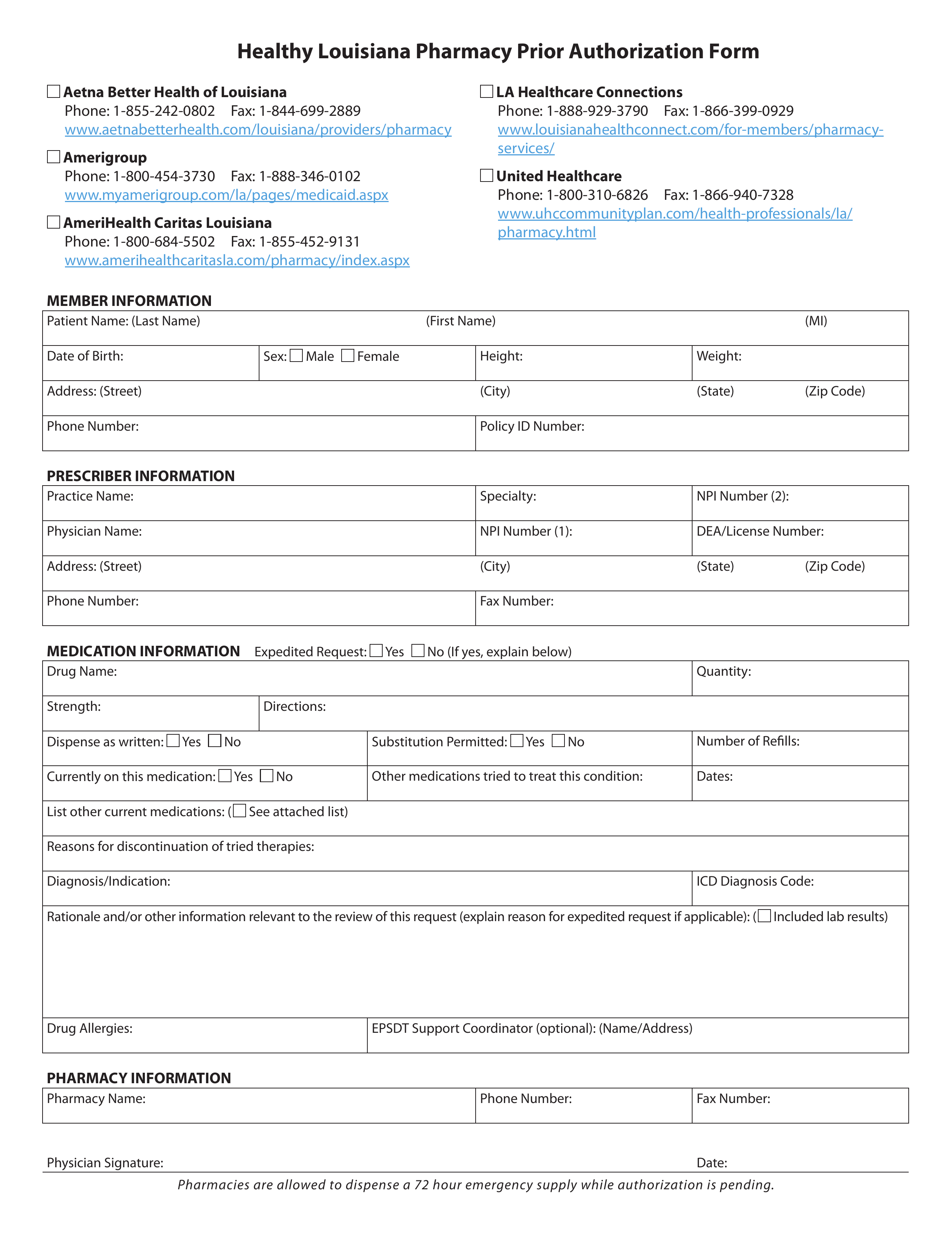
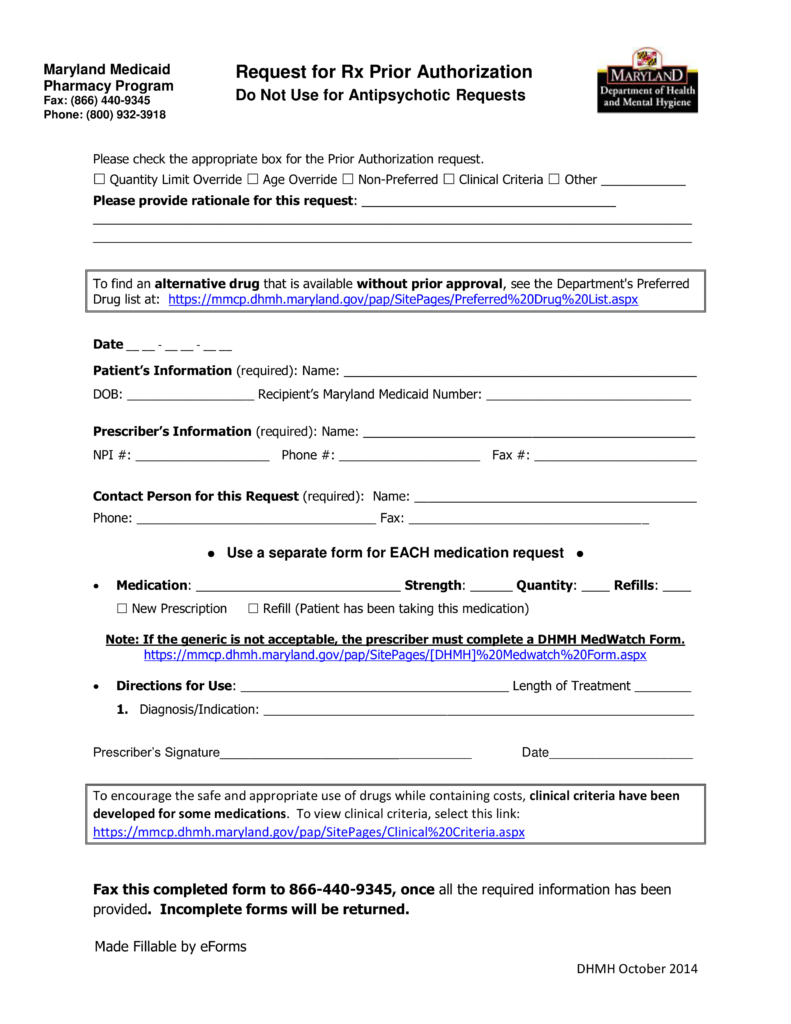
Standard Pharmacy Prior Authorization Form for Prepaid Health Plans
Web arkansas medicaid prior authorization forms | covermymeds manage your arkansas medicaid prior authorization requests our electronic prior authorization (epa). Web arkansas medicaid state supplemental rebate contract template.pdf may 26, 2023 4:17:32 pm certified behavioral health agencies (bha).pdf may 26, 2023 4:32:09 pm. Web watch for your renewal form, fill it out, and return it to arkansas medicaid right away.

What Medicare Form Do I Complete To Revalidate
Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request page 1 of 1 after completing the information below please fax to. Web the following is a list of available prior authorizations forms: Web to become an arkansas medicaid provider, please visit ar medicaid provider enrollment by clicking here. Web send completed form to: This number must.
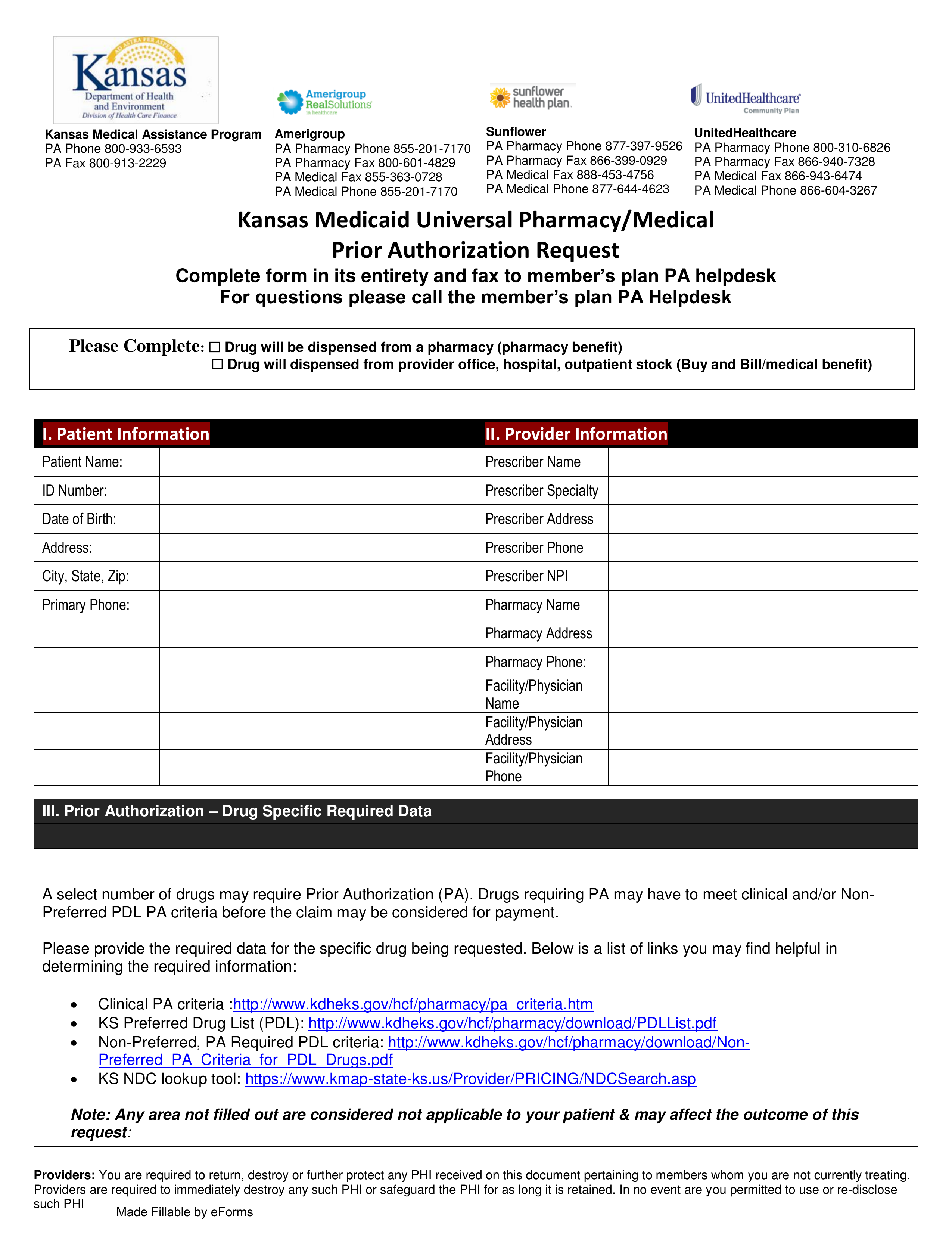
Free Kansas Medicaid Prior (Rx) Authorization Form PDF eForms
Learn more the official website of the state. Easily fill out pdf blank, edit, and sign them. Navigate addt/eidt prior authorization form; If an authorization is needed, you can access our login to submit online. Web to become an arkansas medicaid provider, please visit ar medicaid provider enrollment by clicking here.
Free Alaska Medicaid Prior Rx Authorization Form Pdf Eforms
Web send completed form to: Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request fax form to: Web to become an arkansas medicaid provider, please visit ar medicaid provider enrollment by clicking here. Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request page 1 of 1 after completing the information below please.
Medco Prior Auth Form Medication Form Resume Examples q25Z4Lxk0o
Web outpatient medicaid complete and fax to: 0.4 mb jun 28' 2023. Web send completed form to: We’ll make determinations for prior authorization requests based on unitedhealthcare clinical policy requirements for coverage. Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request fax form to:
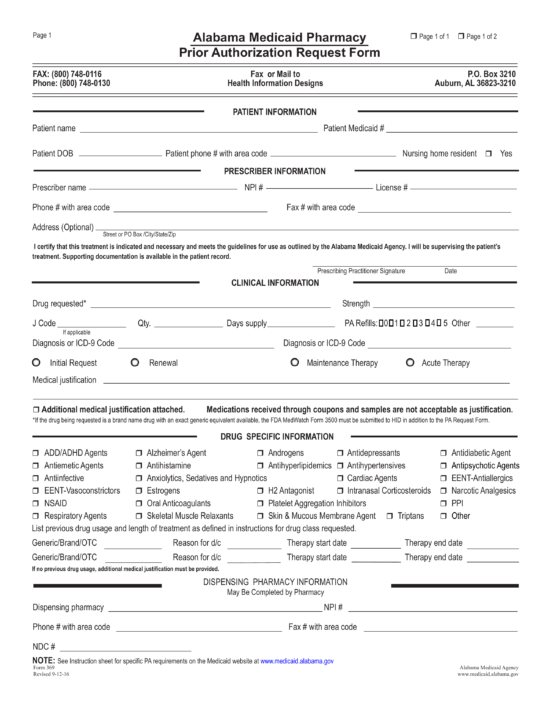
Free Alabama Medicaid Prior (Rx) Authorization Form PDF eForms
Learn more the official website of the state. Information about where to get a supply of the forms and links to samples of. 0.4 mb jun 28' 2023. Web arkansas medicaid state supplemental rebate contract template.pdf may 26, 2023 4:17:32 pm certified behavioral health agencies (bha).pdf may 26, 2023 4:32:09 pm. Comments and help with arkansas.
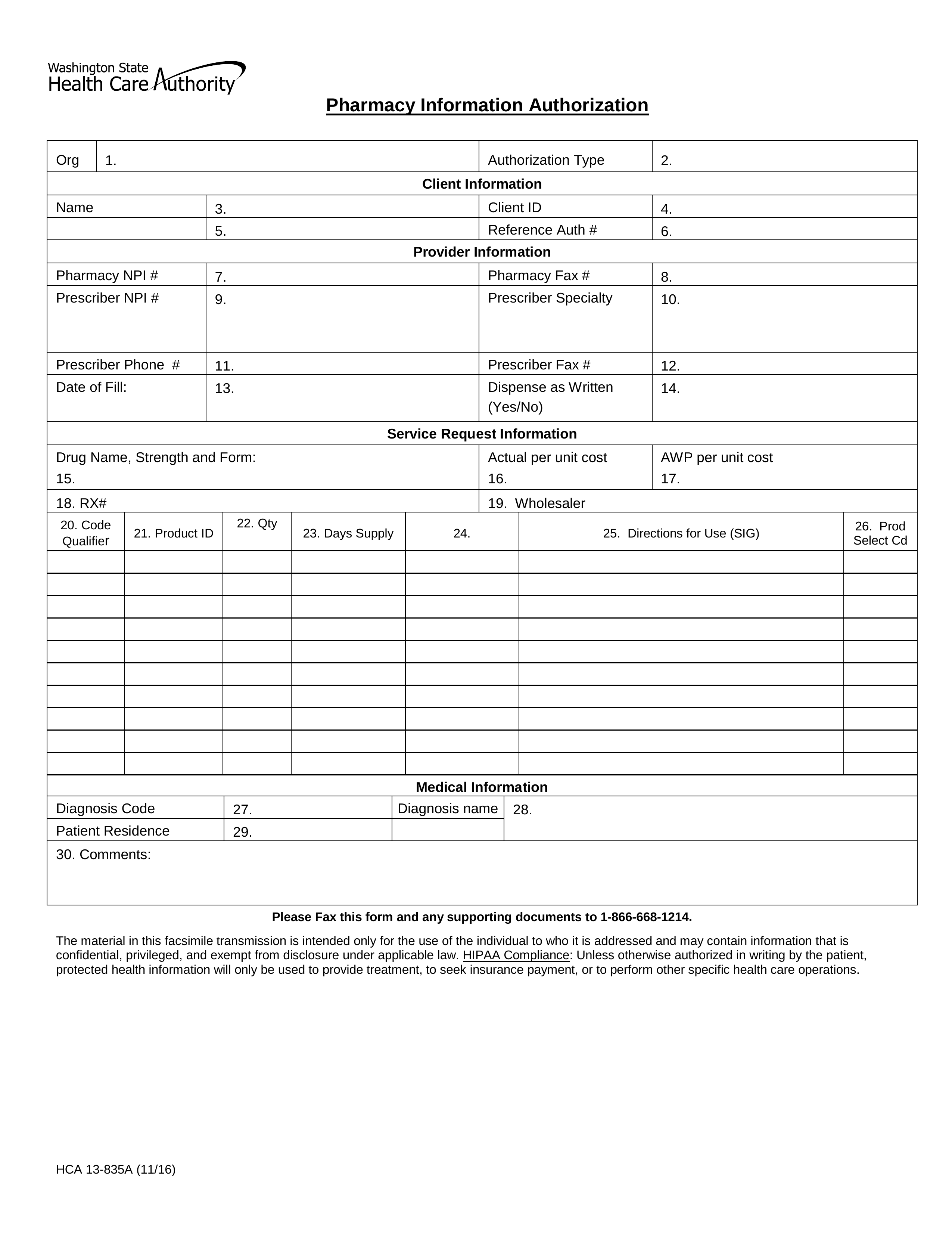
Free Washington Medicaid Prior Authorization Form PDF eForms
Web up to $40 cash back arkansas medicaid prior authorization form is not the form you're looking for? To become a participating provider with empower, please complete the. For extension of benefits for recipients of age 21 or over, send completed pages 1. If an authorization is needed, you can access our login to submit online. Acthar gel (corticotropin injection).
County Care Medicaid Phone Number FLORIDA MEDICAID FILING SERVICES
Save or instantly send your ready. Web inpatient medicaid prior authorization form. Easily fill out pdf blank, edit, and sign them. This number must be entered on the claim form or payment will be denied. For extension of benefits for recipients of age 21 or over, send completed pages 1.
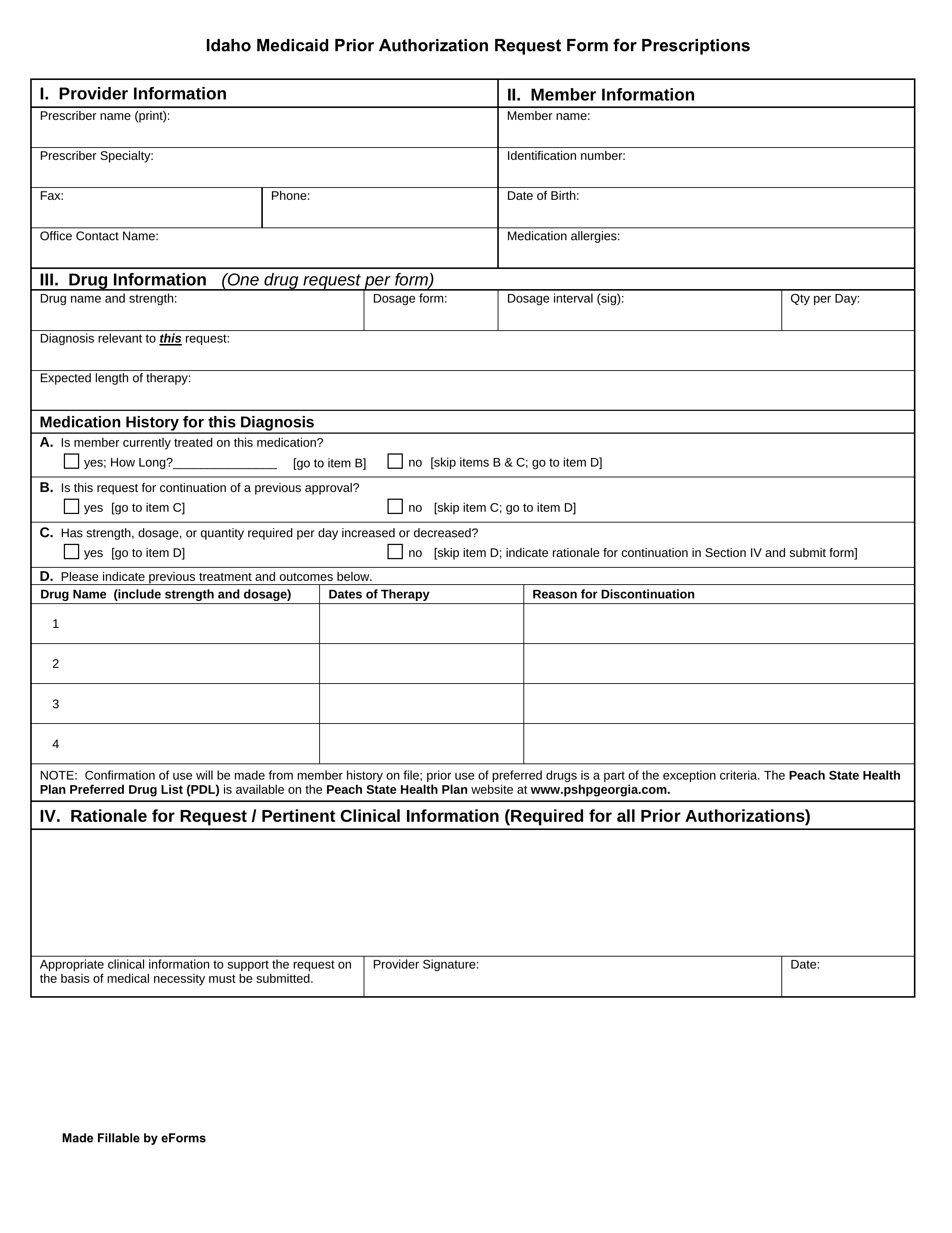
Free Idaho Medicaid Prior (Rx) Authorization Form PDF eForms
Save or instantly send your ready. If an authorization is needed, you can access our login to submit online. Information about where to get a supply of the forms and links to samples of. Easily fill out pdf blank, edit, and sign them. Web arkansas medicaid prior authorization forms | covermymeds manage your arkansas medicaid prior authorization requests our electronic.
Save Or Instantly Send Your Ready.
Web to become an arkansas medicaid provider, please visit ar medicaid provider enrollment by clicking here. Web the following is a list of available prior authorizations forms: We’ll make determinations for prior authorization requests based on unitedhealthcare clinical policy requirements for coverage. Web watch for your renewal form, fill it out, and return it to arkansas medicaid right away to avoid losing medicaid coverage if you are eligible.
Web Arkansas Medicaid Prior Authorization Forms | Covermymeds Manage Your Arkansas Medicaid Prior Authorization Requests Our Electronic Prior Authorization (Epa).
Arkansas foundation for medical care, inc., (afmc) – attn: Navigate aba prior authorization form; Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request page 1 of 1 after completing the information below please fax to. Web what can you do in the provider portal.
If An Authorization Is Needed, You Can Access Our Login To Submit Online.
Search for another form here. Service must be performed before the end of the. 0.4 mb jun 28' 2023. Hepatitis c virus medication therapy request form.
Web Prior Authorization Control Number:
Web send completed form to: Through this secure and easy to use internet portal, healthcare providers can submit claims and inquire on the status of their claims, inquire. Web to prior authorize services for recipients under age 21, send completed pages 1 through 6 to: Web arkansas medicaid prescription drug program statement of medical necessity prior authorization request fax form to: