Aflac Short Term Disability Form
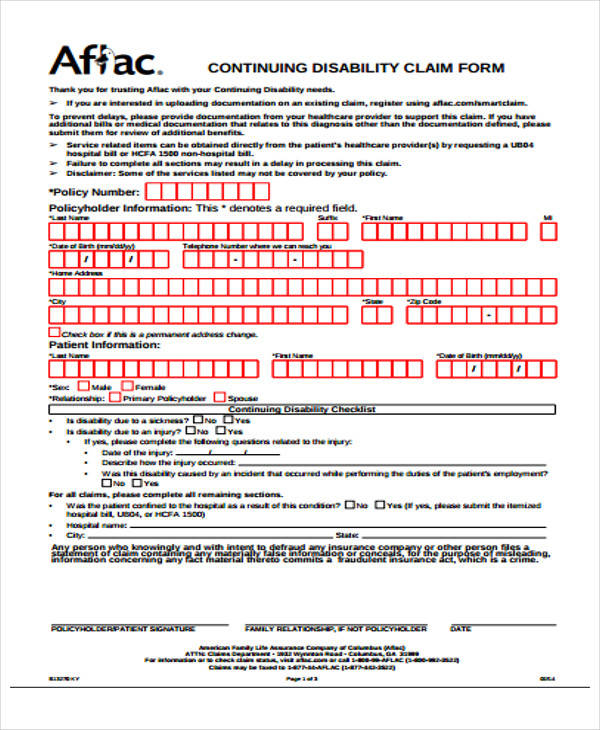
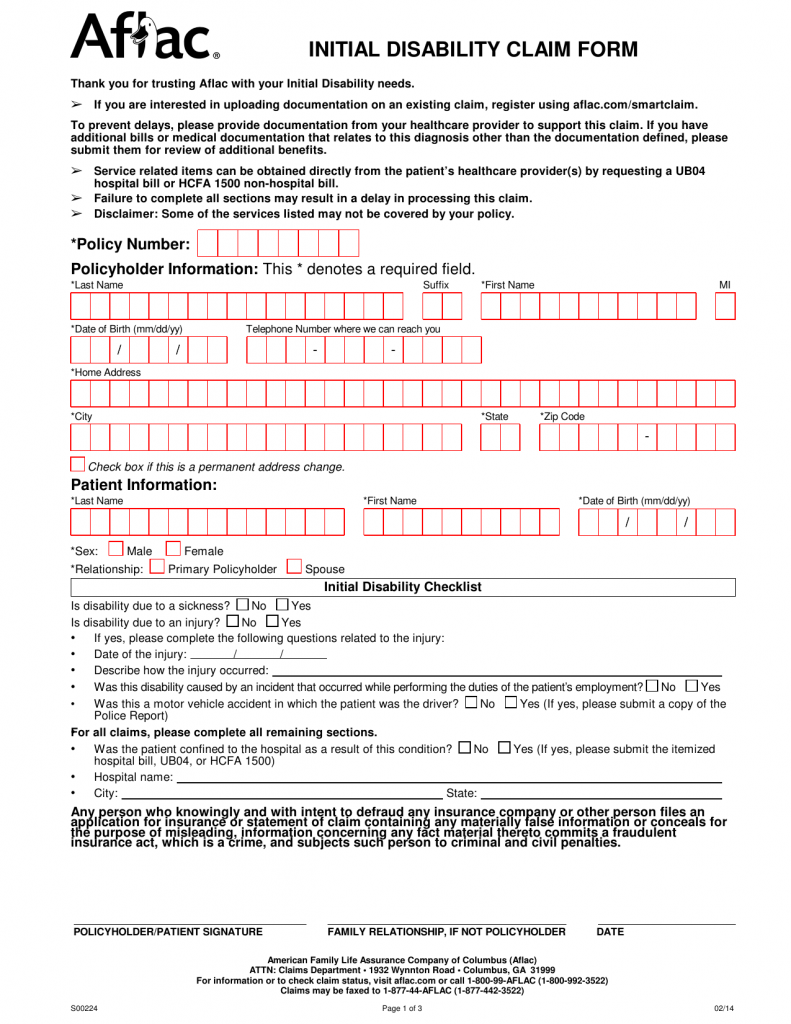
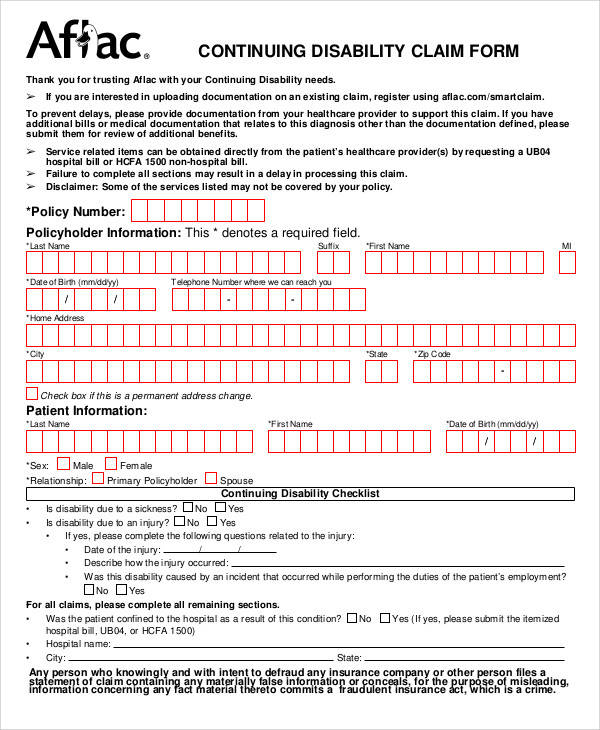
Aflac Short Term Disability Form - Authorization to obtain information (au). Web post office box 84075 * columbus, ga. American family life assurance company of columbus (herein referred to as aflac) You choose the plan that’s right for you based on your financial needs and. Female primary policyholder spouse continuingdisabilitychecklist is. For further information and questions, utilize the. • it’s sold on an individual basis. Aflacs initial claim forms will be used for starting a new claim in the case of a disability due to sickness, injury, or. Web aflac initial short term disability form. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.
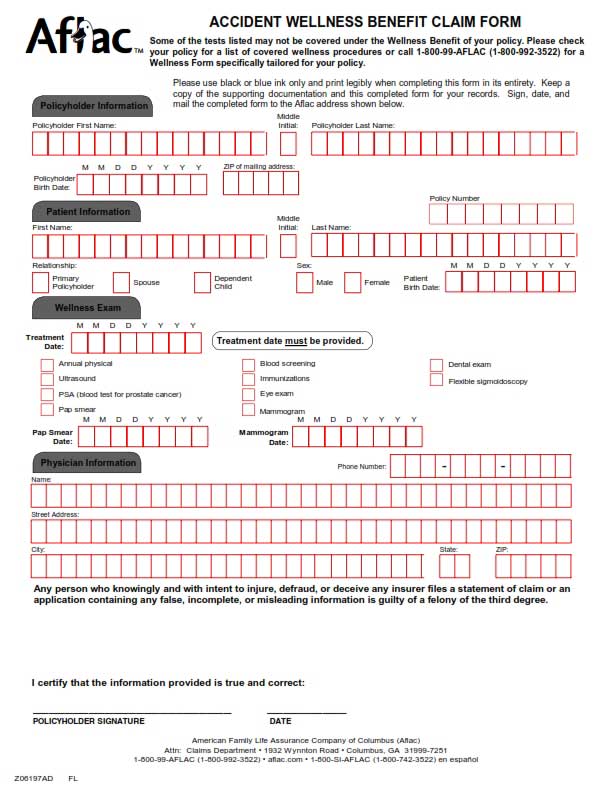
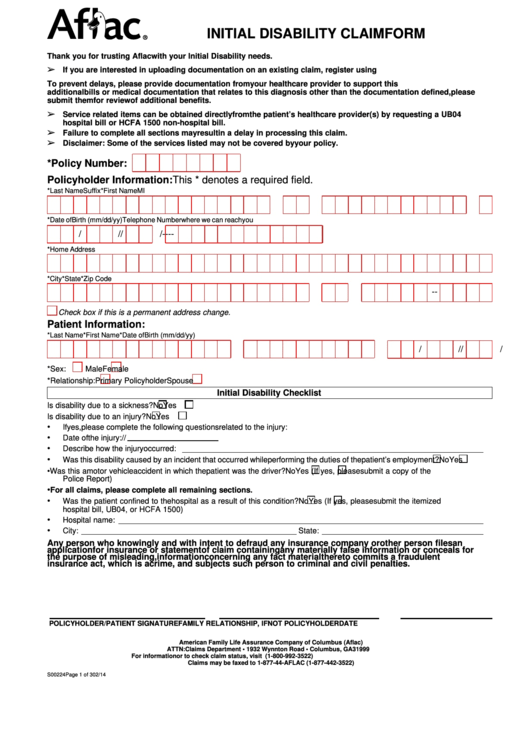
Nt (forms are to be completed on or after disability date to avoid. *last name *first name *date of birth (mm/dd/yy) / / *sex: Aflacs initial claim forms will be used for starting a new claim in the case of a disability due to sickness, injury, or. What if a disability interrupted. Web form a57375cb2nj ic(8/10) the need becoming disabled is often an unexpected and burdensome experience, and it can happen to anyone. Web ub04 (itemized hospital bill). Web post office box 84075 * columbus, ga. (this allows aflac to request additional. Authorization to obtain information (au). You choose the plan that’s right for you based on your financial needs and.
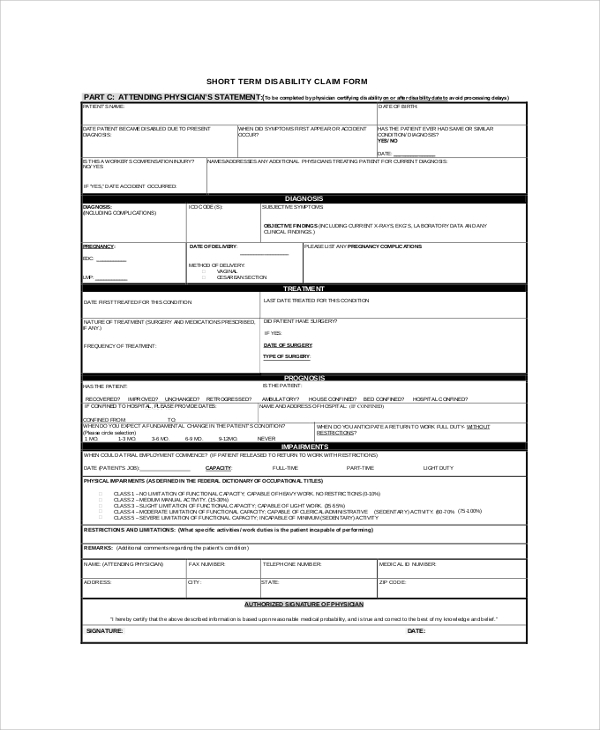
Web aflac initial short term disability form. American family life assurance company of columbus (herein referred to as aflac) • it’s sold on an individual basis. Web post office box 84075 * columbus, ga. Nt (forms are to be completed on or after disability date to avoid. Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the. You may access the claim forms without logging in by selecting “glossary” and typing “claim form” into the search box. Aflacs initial claim forms will be used for starting a new claim in the case of a disability due to sickness, injury, or. Please sign and return the attached hipaa. You choose the plan that’s right for you based on your financial needs and.
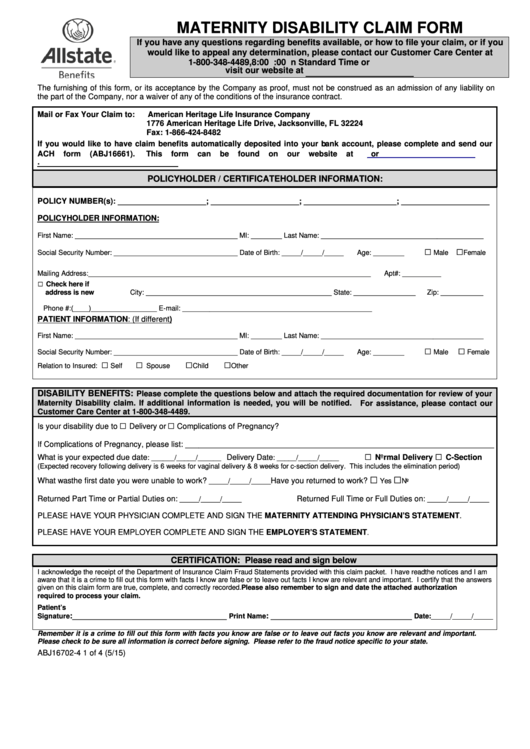
Form Abj167024 Maternity Disability Claim Form 2015 printable pdf
What if a disability interrupted. (this allows aflac to request additional. Please sign and return the attached hipaa. • it’s sold on an individual basis. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.
FREE 50+ Sample Claim Forms in PDF MS Word
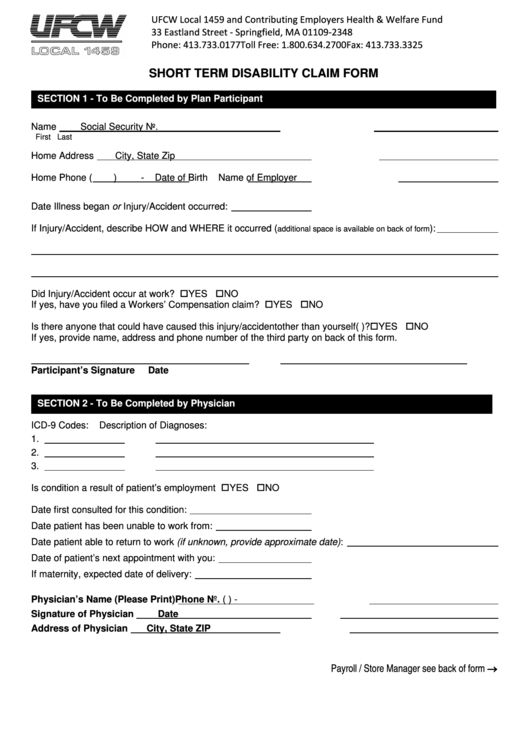
You may access the claim forms without logging in by selecting “glossary” and typing “claim form” into the search box. Aflacs initial claim forms will be used for starting a new claim in the case of a disability due to sickness, injury, or. Web short term disability claim form. Nt (forms are to be completed on or after disability date.
Download Aflac Short Term Disability Claim Form/ Initial Disability
For further information and questions, utilize the. Web aflac initial short term disability form. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Web short term disability claim form. What if a disability interrupted.
FREE 42+ Sample Claim Forms in PDF
Please sign and return the attached hipaa. Female primary policyholder spouse continuingdisabilitychecklist is. • it’s sold on an individual basis. *last name *first name *date of birth (mm/dd/yy) / / *sex: What if a disability interrupted.

Gallery of Aflac Short Term Disability forms Best Of Membership Benefits
You choose the plan that’s right for you based on your financial needs and. Web aflac initial short term disability form. Authorization to obtain information (au). Female primary policyholder spouse continuingdisabilitychecklist is. Aflacs initial claim forms will be used for starting a new claim in the case of a disability due to sickness, injury, or.
FREE 8+ Sample Aflac Claim Forms in PDF
You choose the plan that’s right for you based on your financial needs and. Web form a57375cb2nj ic(8/10) the need becoming disabled is often an unexpected and burdensome experience, and it can happen to anyone. Female primary policyholder spouse continuingdisabilitychecklist is. You may access the claim forms without logging in by selecting “glossary” and typing “claim form” into the search.
Aflac Claim Forms Printable Master of Documents
(this allows aflac to request additional. Female primary policyholder spouse continuingdisabilitychecklist is. Web ub04 (itemized hospital bill). You may access the claim forms without logging in by selecting “glossary” and typing “claim form” into the search box. American family life assurance company of columbus (herein referred to as aflac)
Is Aflac Short Term Disability Taxable
Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the. Web post office box 84075 * columbus, ga. Web short term disability claim form. What if a disability interrupted. Web life claim forms for the state of illinois must be obtained by contacting aflac.

Fill Free fillable Aflac Insurance PDF forms
Web form a57375cb2nj ic(8/10) the need becoming disabled is often an unexpected and burdensome experience, and it can happen to anyone. • it’s sold on an individual basis. Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the. (this allows aflac to request additional..
Cincinnati Ins Co Claims Aflac Injury Claim
Web form a57375cb2nj ic(8/10) the need becoming disabled is often an unexpected and burdensome experience, and it can happen to anyone. Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the. Nt (forms are to be completed on or after disability date to avoid..
Web Aflac Initial Short Term Disability Form.
American family life assurance company of columbus (herein referred to as aflac) Web post office box 84075 * columbus, ga. Authorization to obtain information (au). For further information and questions, utilize the.
Aflacs Initial Claim Forms Will Be Used For Starting A New Claim In The Case Of A Disability Due To Sickness, Injury, Or.
What if a disability interrupted. Web short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Nt (forms are to be completed on or after disability date to avoid.
Female Primary Policyholder Spouse Continuingdisabilitychecklist Is.
Web form a57375cb2nj ic(8/10) the need becoming disabled is often an unexpected and burdensome experience, and it can happen to anyone. (this allows aflac to request additional. You may access the claim forms without logging in by selecting “glossary” and typing “claim form” into the search box. You choose the plan that’s right for you based on your financial needs and.
• It’s Sold On An Individual Basis.
Web ub04 (itemized hospital bill). Please sign and return the attached hipaa. *last name *first name *date of birth (mm/dd/yy) / / *sex: Web short term disability claim form.