Wellcare Provider Dispute Form
Wellcare Provider Dispute Form - Web you can dispute a claim with a status of fullypaid. All fields are required information: All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. Choose the paid line items you want to dispute. If you are having difficulties registering please. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. You can even print your chat history to reference later! Helpful resources essential plans provider manual Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration.
You can even print your chat history to reference later! A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. If you are having difficulties registering please. Web you can dispute a claim with a status of fullypaid. All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. From the select action drop down, choose dispute claim. Use the claims search option to find the claim. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Web if you provide services such as home health, personal care services, hospice, dme, inpatient services and more, please download and complete the forms below:
Helpful resources essential plans provider manual Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web access key forms for authorizations, claims, pharmacy and more. Web if you provide services such as home health, personal care services, hospice, dme, inpatient services and more, please download and complete the forms below: Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english dme authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. From the select action drop down, choose dispute claim. You can even print your chat history to reference later! All fields are required information a request for reconsideration (level i) the manner in which a claim was processed.
Dispute Form Medicare Fill Online, Printable, Fillable, Blank pdfFiller
You can even print your chat history to reference later! All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english dme authorization.
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. You can even print your chat history to reference later! A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Is a communication from the provider about a disagreement with a claim.
Wellcare Appeal Form Fill Out and Sign Printable PDF Template signNow
If you are having difficulties registering please. All fields are required information: Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration. Web disputes, reconsiderations and grievances. Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor.

Medicaid Providers WellCare
Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. If you are having difficulties registering please. You can even print your chat history to reference later! Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web if you provide services such as.
Fillable Kentucky Medicaid Mco Member Grievance Form printable pdf download
Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english dme authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a.
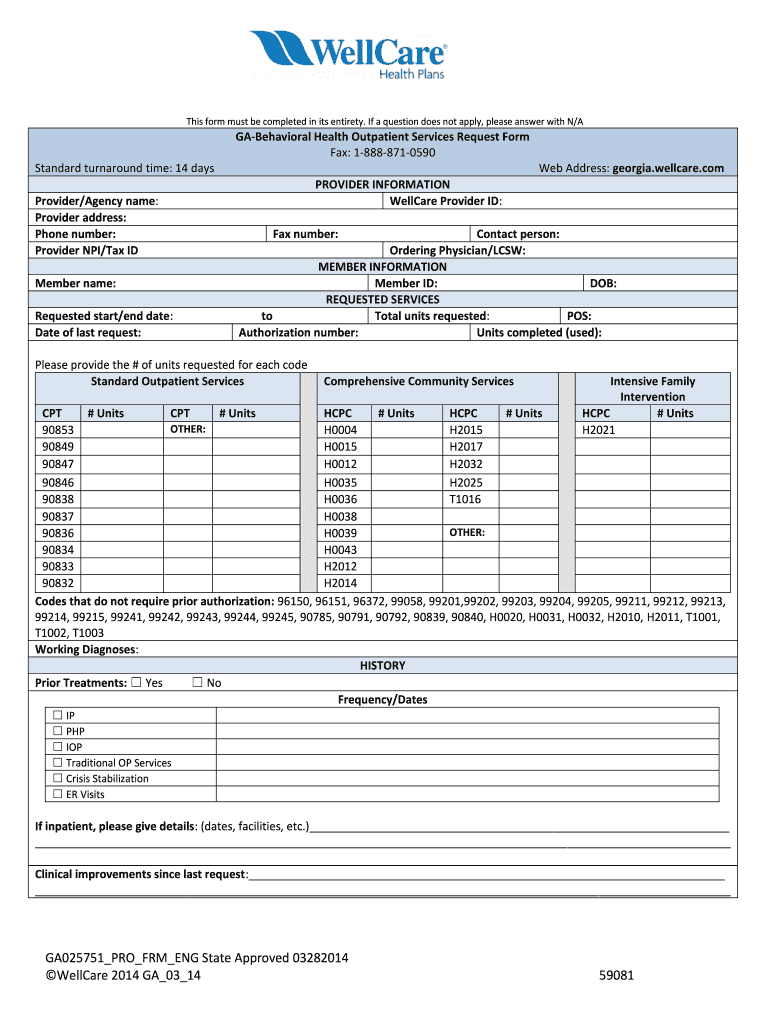
Wellcare Behavioral Health Service Request Form Fill Out and Sign
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. A request for reconsideration (level i) is a communication from the provider about a disagreement on how a claim was processed. Web disputes, reconsiderations and grievances. Web you can dispute a claim with a status of fullypaid. All fields are required information:

wellcare reimbursement form Fill out & sign online DocHub
If you are having difficulties registering please. Choose the paid line items you want to dispute. Use the claims search option to find the claim. All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. Web use this form as part of the wellcare by allwell request for reconsideration and claim.

Wellcare letter of intent form Fill out & sign online DocHub
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Web you can dispute a claim with a status of fullypaid. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Use the claims search option to find the claim. Helpful resources essential plans provider.

Free PDF, DOC Format Download Free & Premium Templates Daycare
Web you can dispute a claim with a status of fullypaid. Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english dme authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english. Send this form with all pertinent medical.

Wellcare Part D Enrollment Form Form Resume Examples WjYDLNMYKB
If you are having difficulties registering please. Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration. Web if you provide services such as home health, personal care services, hospice, dme, inpatient services and more, please download and complete the forms below: Web you can dispute a claim with a status of.
If You Are Having Difficulties Registering Please.
From the select action drop down, choose dispute claim. Is a communication from the provider about a disagreement with a claim dispute (level ii) request for reconsideration. Web disputes, reconsiderations and grievances. Web provider payment dispute ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider reconsideration request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english provider waiver of liability (wol) ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english authorization forms delegated vendor request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english dme authorization request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english home health services request ꭱꮃꮧꮯ ꭶꮲꮝꭼꭲ english.
Use The Claims Search Option To Find The Claim.
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. Web you can dispute a claim with a status of fullypaid. Web if you provide services such as home health, personal care services, hospice, dme, inpatient services and more, please download and complete the forms below: All fields are required information:
A Request For Reconsideration (Level I) Is A Communication From The Provider About A Disagreement On How A Claim Was Processed.
Send this form with all pertinent medical documentation to support the request to wellcare health plans, inc. You can even print your chat history to reference later! Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Choose the paid line items you want to dispute.
Web Use This Form As Part Of The Wellcare By Allwell Request For Reconsideration And Claim Dispute Process.
Helpful resources essential plans provider manual All fields are required information a request for reconsideration (level i) the manner in which a claim was processed. Web access key forms for authorizations, claims, pharmacy and more.