Optumrx Tier Exception Form
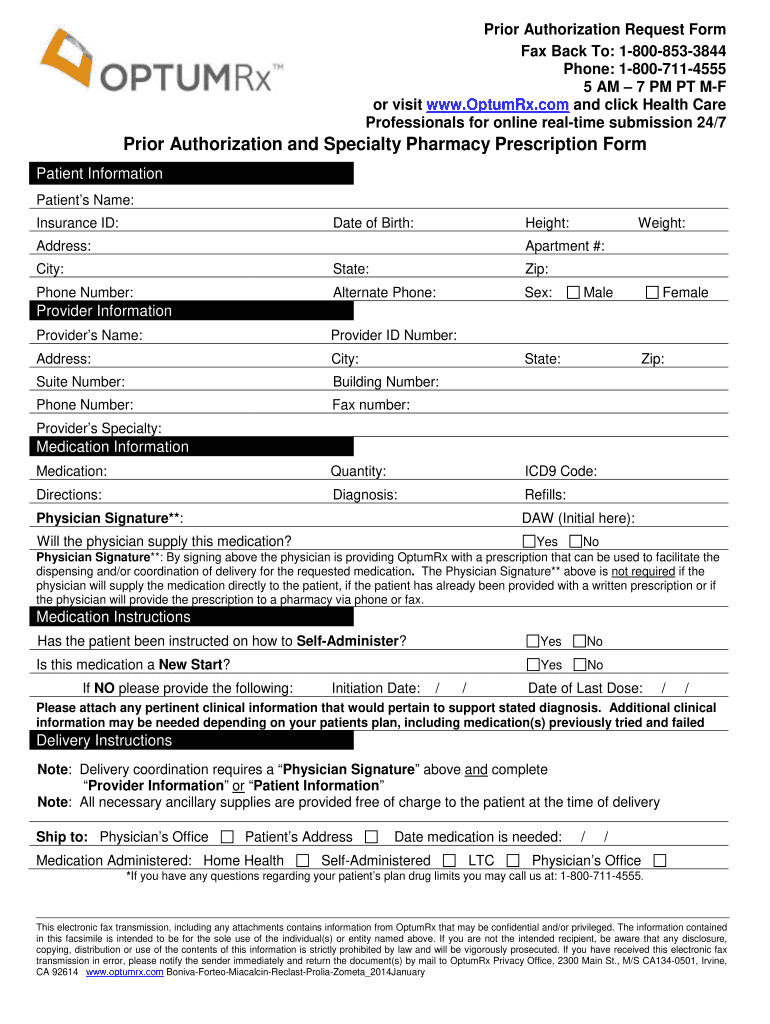
Optumrx Tier Exception Form - Please fill out all applicable sections on both pages completely and legibly. Member information (required) provider information (required) member name: Use the cross or check marks in the top toolbar to select your answers in the list boxes. Do not copy for future use. Include the date to the form using the date feature. Use get form or simply click on the template preview to open it in the editor. You can ask the plan to cover your drug even if it is not on the plan's drug list (formulary). Web partial copay waiver (pcw) exception prior authorization request form. Web to submit a tiering exception, copay waiver, tier cost sharing, or any other cost reductions requests (e.g., hcr), please contact the optumrx® pa department through telephone or fax. Web fill out every fillable field.
Web optumrx tier exception form is a request form that allows a patient to request a medication that is a higher tier on their insurance formulary. Start completing the fillable fields and carefully type in required information. Click on the sign tool and make a signature. Web to submit a tiering exception, copay waiver, tier cost sharing, or any other cost reductions requests (e.g., hcr), please contact the optumrx® pa department through telephone or fax. Member information (required) provider information (required) member name: Who may make a request: Optumrx is not authorized to review requests for medications supplied by the physician’s office. Forms are updated frequently and may be barcoded Web fill out every fillable field. You may also ask us for a coverage determination by calling the member services number on the back of your id card.
Include the date to the form using the date feature. Web partial copay waiver (pcw) exception prior authorization request form. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Your plan may have multiple or no tiers. Generic medications are shown in lowercase (for example, clobetasol). You can ask the plan to cover your drug even if it is not on the plan's drug list (formulary). Web this form may be sent to us by mail or fax: Click on the sign tool and make a signature. Who may make a request: Member information (required) provider information (required) member name:
Optumrx Medicare Part D Tier Exception Form Form Resume Examples
Use get form or simply click on the template preview to open it in the editor. Optumrx is not authorized to review requests for medications supplied by the physician’s office. You may also ask us for a coverage determination by calling the member services number on the back of your id card. Web to submit a tiering exception, copay waiver,.
Optum Rx Pa Form Fill Out and Sign Printable PDF Template signNow
Forms are updated frequently and may be barcoded. Please fill out all applicable sections on both pages completely and legibly. Generic medications are shown in lowercase (for example, clobetasol). Web this form may be sent to us by mail or fax: Forms are updated frequently and may be barcoded
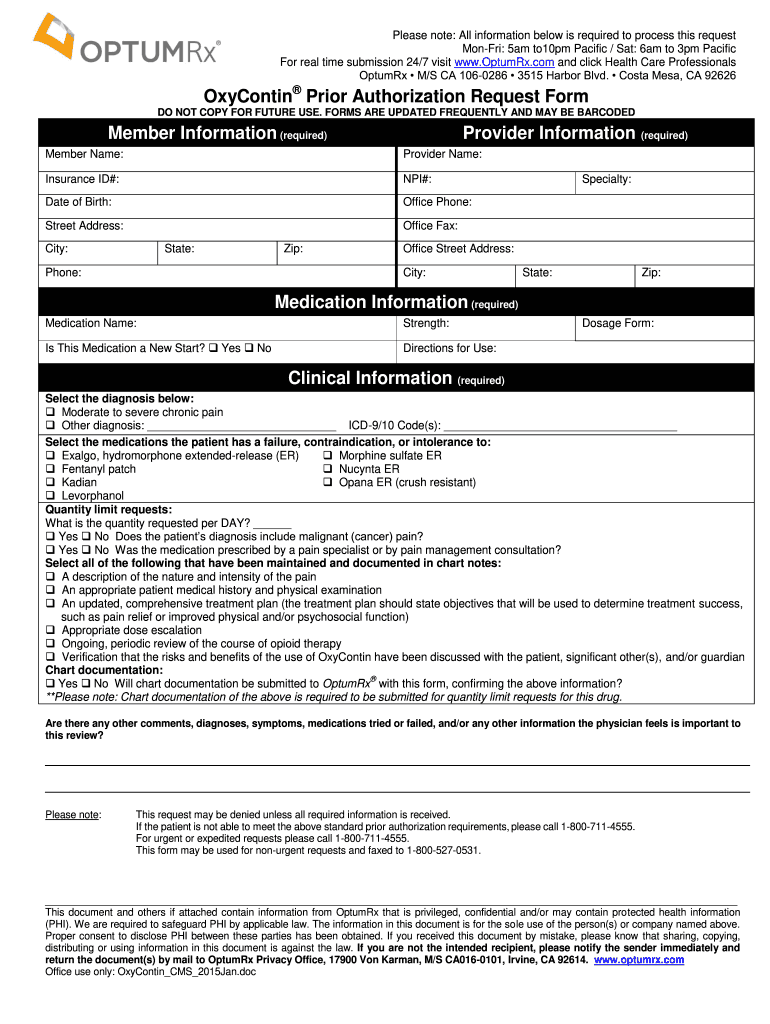
Optum rx oxycontin pa form Fill Out and Sign Printable PDF Template
Generic medications are shown in lowercase (for example, clobetasol). Include the date to the form using the date feature. Web optumrx tier exception form is a request form that allows a patient to request a medication that is a higher tier on their insurance formulary. Please fill out all applicable sections on both pages completely and legibly. You may also.

2014 OPTUMRx Nuvigil & Provigil Prior Authorization Request Form Fill
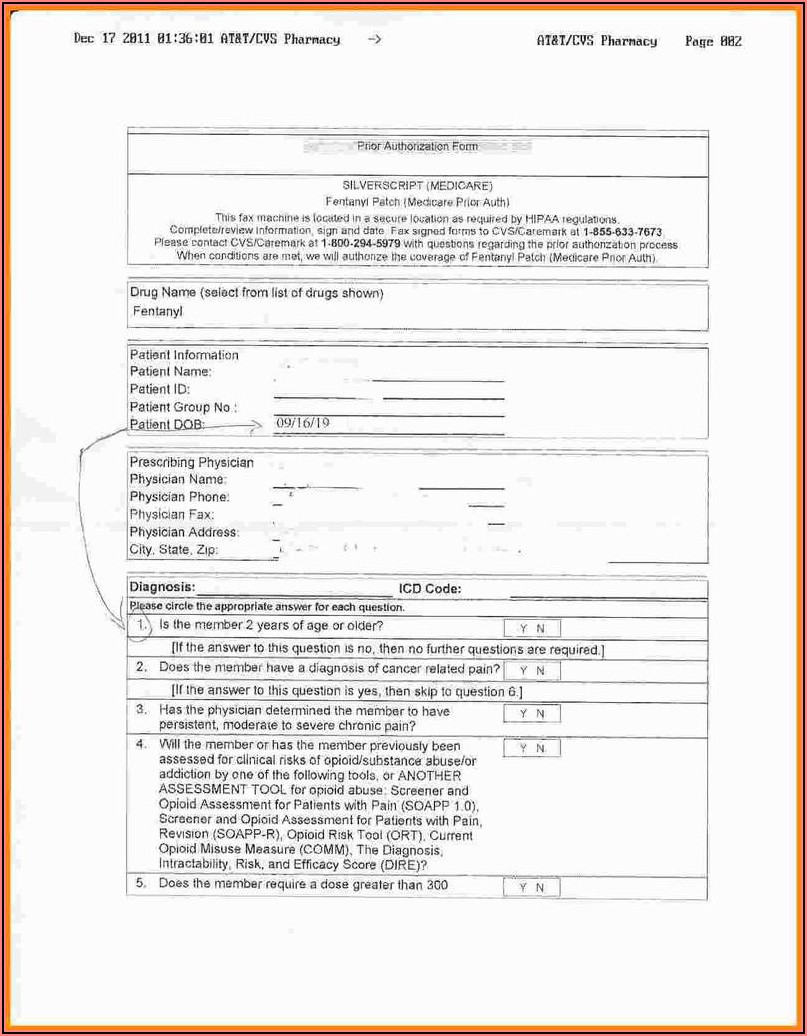
Do not copy for future use. Use get form or simply click on the template preview to open it in the editor. Optumrx is not authorized to review requests for medications supplied by the physician’s office. Web partial copay waiver (pcw) exception prior authorization request form. Web prescription drug prior authorization or step therapy exception request form patient name:

Optumrx Medicare Part D Electronic Prior Authorization form Brilliant
Web prescription drug prior authorization or step therapy exception request form patient name: Web this form may be sent to us by mail or fax: Who may make a request: Use get form or simply click on the template preview to open it in the editor. Include the date to the form using the date feature.
Optumrx Prior Authorization Form Cialis Rx Prior Authorization
You may also ask us for a coverage determination by calling the member services number on the back of your id card. Web partial copay waiver (pcw) exception prior authorization request form. Web optumrx tier exception form is a request form that allows a patient to request a medication that is a higher tier on their insurance formulary. Web to.

Cvs Caremark Tier Exception Form
Do not copy for future use. Your plan may have multiple or no tiers. You can ask the plan to cover your drug even if it is not on the plan's drug list (formulary). Web optumrx tier exception form is a request form that allows a patient to request a medication that is a higher tier on their insurance formulary..
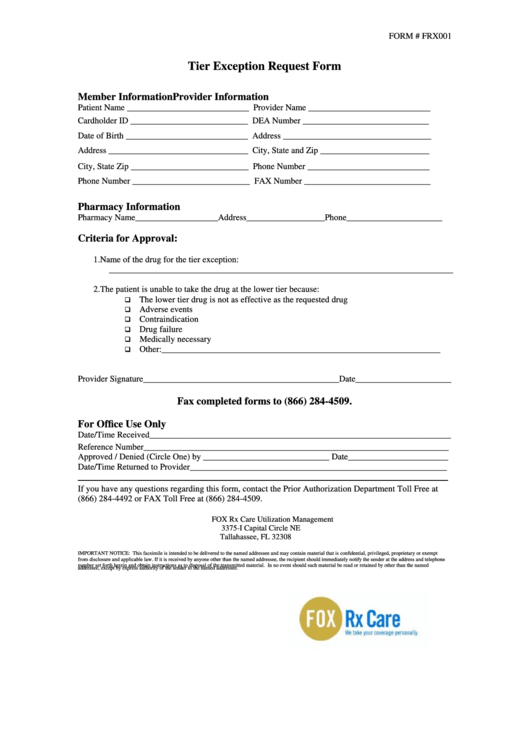
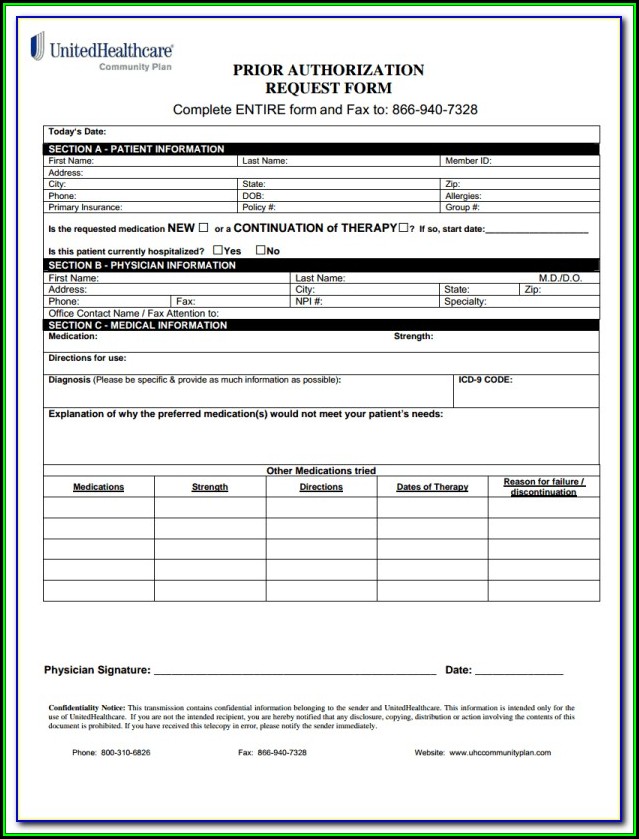
Form Frx001 Tier Exception Request Form printable pdf download
Generic medications are shown in lowercase (for example, clobetasol). You can ask the plan to cover your drug even if it is not on the plan's drug list (formulary). You may also ask us for a coverage determination by calling the member services number on the back of your id card. Your plan may have multiple or no tiers. Include.
Optumrx Prior Authorization Form Cialis — Pharmacy General Exception Forms
Please fill out all applicable sections on both pages completely and legibly. Start completing the fillable fields and carefully type in required information. You may also ask us for a coverage determination by calling the member services number on the back of your id card. Web this form may be sent to us by mail or fax: Do not copy.
Optumrx Medicare Part D Tier Exception Form Form Resume Examples
You may also ask us for a coverage determination by calling the member services number on the back of your id card. Generic medications are shown in lowercase (for example, clobetasol). Web this form may be sent to us by mail or fax: Include the date to the form using the date feature. Use get form or simply click on.
Forms Are Updated Frequently And May Be Barcoded.
Optumrx is not authorized to review requests for medications supplied by the physician’s office. Web prescription drug prior authorization or step therapy exception request form patient name: You can ask the plan to cover your drug even if it is not on the plan's drug list (formulary). Generic medications are shown in lowercase (for example, clobetasol).
Use The Cross Or Check Marks In The Top Toolbar To Select Your Answers In The List Boxes.
Who may make a request: Include the date to the form using the date feature. Web optumrx tier exception form is a request form that allows a patient to request a medication that is a higher tier on their insurance formulary. Start completing the fillable fields and carefully type in required information.
Your Plan May Have Multiple Or No Tiers.
Use get form or simply click on the template preview to open it in the editor. You can't ask for an exception to the copayment or coinsurance amount you're required to pay for the drug. Please fill out all applicable sections on both pages completely and legibly. Web partial copay waiver (pcw) exception prior authorization request form.
Forms Are Updated Frequently And May Be Barcoded
Web to submit a tiering exception, copay waiver, tier cost sharing, or any other cost reductions requests (e.g., hcr), please contact the optumrx® pa department through telephone or fax. Web fill out every fillable field. Do not copy for future use. Member information (required) provider information (required) member name: