Molina Reconsideration Form
Molina Reconsideration Form - ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Please send corrected claims as a normal claim submission electronically or via the availity essentials portal. Easily fill out pdf blank, edit, and sign them. Download preservice appeal request form. Medicaid, medicare, dual snp post claim: This includes attachments for coordination of benefits (cob) or itemized statements. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. Web marketplace provider reconsideration request form today’s date: Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow 30 days to process this reconsideration request number of faxed pages (including cover sheet): Download claim reconsideration request form.
/ / (*) attach required documentation or proof to support. ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Incomplete forms will not be processed and returned to submitter. Save or instantly send your ready documents. This includes attachments for coordination of benefits (cob) or itemized statements. Medicaid, medicare, dual snp post claim: Easily fill out pdf blank, edit, and sign them. Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. Web complete molina reconsideration form online with us legal forms. Please refer to your molina provider manual.
Incomplete forms will not be processed and returned to submitter. Incomplete forms will not be processed. Please send corrected claims as a normal claim submission electronically or via the availity essentials portal. / / (*) attach required documentation or proof to support. Download claim reconsideration request form. Please refer to your molina provider manual. ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. Medicaid, medicare, dual snp post claim: Download preservice appeal request form.

Washington Molina Marketplace Appeal Request Form. Washington Molina
Incomplete forms will not be processed and returned to submitter. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information. • availity essentials portal appeal process • verbally (medicaid line of business): Please refer to your molina provider manual. Please send corrected claims as a normal claim submission electronically or via the.

What Is Texas Help Medicare Medicaid
Download claim reconsideration request form. Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow 30 days to process this reconsideration request number of faxed pages (including cover sheet): Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. Easily fill out pdf blank, edit, and.
Colorado Request for Reconsideration Form Download Printable PDF
Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. Web marketplace provider reconsideration request form today’s date: Incomplete forms will not be processed and returned to submitter. Easily fill out pdf blank, edit, and sign them. Download claim reconsideration request form.

Aarp Medicare Part D Medication Prior Authorization Form Form
Save or instantly send your ready documents. Medicaid, medicare, dual snp post claim: Incomplete forms will not be processed. Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. This includes attachments for coordination of benefits (cob) or itemized statements.

Molina Broker Reconciliation Form YouTube
Web complete molina reconsideration form online with us legal forms. Please send corrected claims as a normal claim submission electronically or via the availity essentials portal. Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow 30 days to process this reconsideration request number of faxed pages (including cover sheet):.
Virginia Provider Claim Reconsideration Form printable pdf download
Web complete molina reconsideration form online with us legal forms. • availity essentials portal appeal process • verbally (medicaid line of business): ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Please refer to your molina provider manual. Incomplete forms will not be.
Molina Prior Authorization Form 2021 Fill Online, Printable, Fillable
This includes attachments for coordination of benefits (cob) or itemized statements. Medicaid, medicare, dual snp post claim: Web complete molina reconsideration form online with us legal forms. Easily fill out pdf blank, edit, and sign them. ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims.
Aarp Printable Application Pdf Fill Online, Printable, Fillable
** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow 30 days to process this reconsideration request number of faxed pages (including cover sheet):.
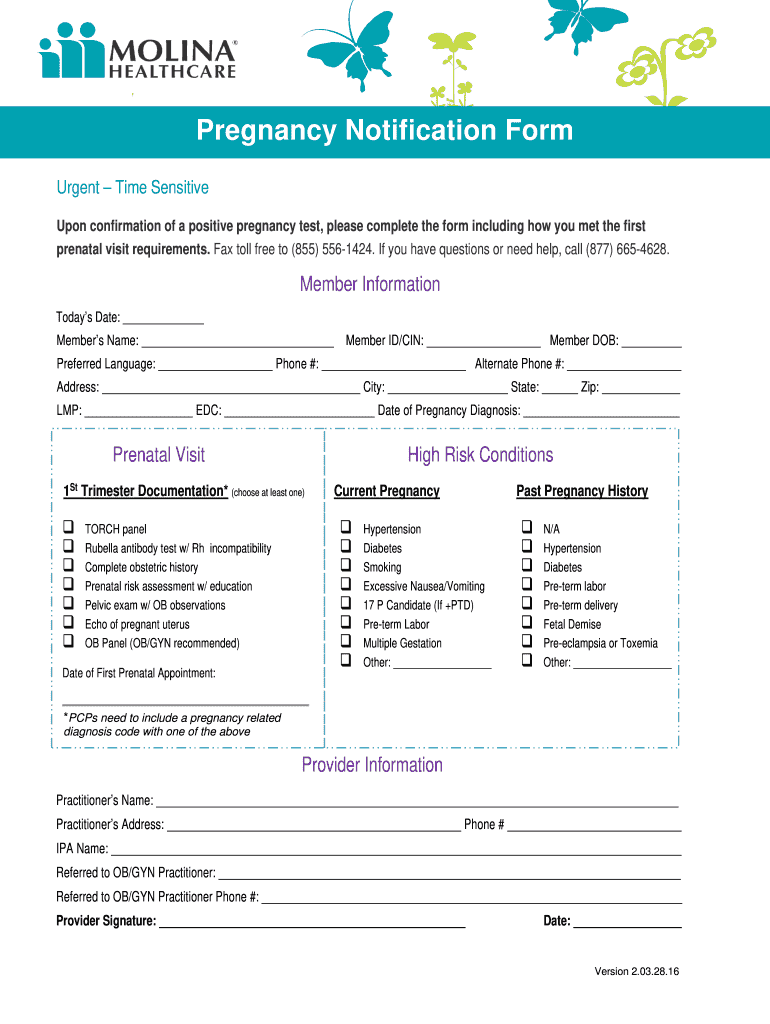
Molina Healthcare Pregnancy Notification Form 20162021 Fill and Sign
Please send corrected claims as a normal claim submission electronically or via the availity essentials portal. Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. / / (*) attach required documentation or proof to support. Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow.

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 September 16, 2011
Web complete molina reconsideration form online with us legal forms. This includes attachments for coordination of benefits (cob) or itemized statements. ** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Easily fill out pdf blank, edit, and sign them. Please refer to your.
Save Or Instantly Send Your Ready Documents.
Web marketplace provider reconsideration request form today’s date: Incomplete forms will not be processed and returned to submitter. Easily fill out pdf blank, edit, and sign them. This includes attachments for coordination of benefits (cob) or itemized statements.
Web Complete Molina Reconsideration Form Online With Us Legal Forms.
** if molina healthcare of south carolina determines there is a system confguration error, a claim analysis will be conducted to pull impacted claims for reprocessing. Web claims reconsideration request form (requests must be received within 120 days of date of original remittance advice) please allow 30 days to process this reconsideration request number of faxed pages (including cover sheet): Please check the applicable reason(s) for the claim reconsideration and attach all supporting documentation. Please refer to your molina provider manual.
Incomplete Forms Will Not Be Processed.
/ / (*) attach required documentation or proof to support. • availity essentials portal appeal process • verbally (medicaid line of business): Please send corrected claims as a normal claim submission electronically or via the availity essentials portal. Web by submitting my information via this form, i consent to having molina healthcare collect my personal information.
Download Claim Reconsideration Request Form.
Download preservice appeal request form. Medicaid, medicare, dual snp post claim: