How To Fill Out Medi-Cal Redetermination Form
How To Fill Out Medi-Cal Redetermination Form - Web there are 2 ways that a party can request a redetermination: Complete and return the form; Web fill out and turn in the enclosed annual redetermination form. Click the green arrow with the inscription next to move from one field to. Specific service (s) and/or item (s) for which a redetermination is being requested. Sign and date on the declaration and signature page î step 3. Web î step 1.read the form and answer the questions î step 2. Web the length of the pauses varies by state and depends on the speed at which it can remedy its problem, said tsai, noting that some states are taking an extra 90 days to correct their systems. You may need to complete a renewal form. Specific date (s) of service.
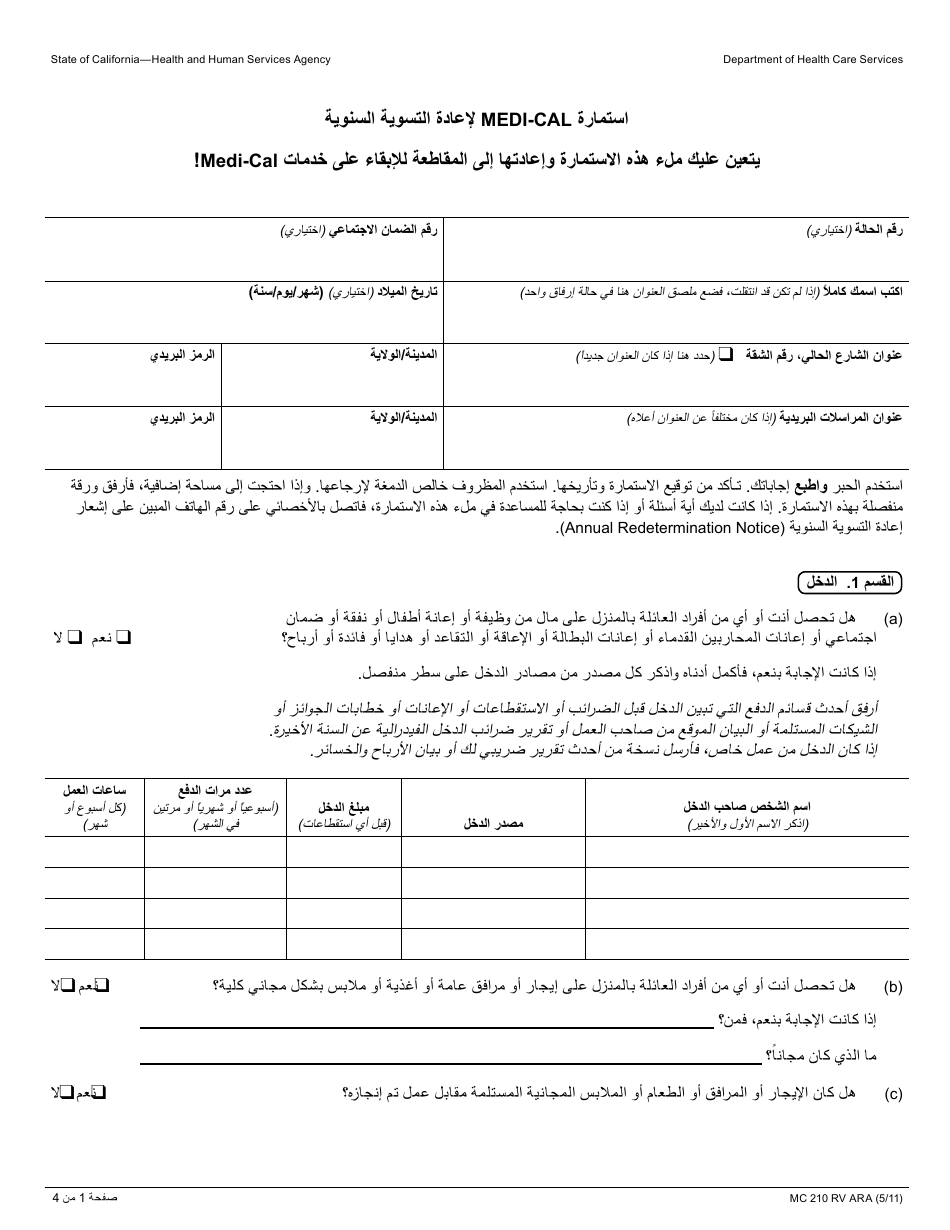
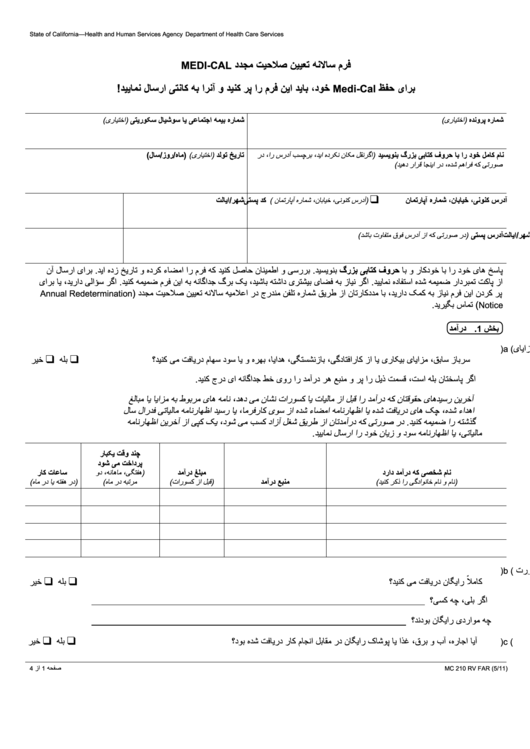
Health insurance premium program (hipp) application. Web fill out and turn in the enclosed annual redetermination form. Web here’s how it works: Complete and return the form; Case number social security number (optional) print your full name birth date (optional) (mm/dd/yyyy) current street address, apartment number city/state zip code mailing address city/state zip code Health insurance premium payment program. If you have any questions or need help filling out this form, call your worker at the telephone number listed on the annual redetermination notice. Make a written request containing all of the following information: Make a written request containing all of the following information: By mail in the envelope that came with this letter.
Beneficiary’s name (first, middle, last) medicare number. Can help you complete this application during the interview if you did not fill out all sections or if you need to make changes. Specific service (s) and/or item (s) for which a redetermination is being requested. Click the green arrow with the inscription next to move from one field to. Respond to the appointment letter; Date the service or item was received (mm/dd/yyyy) item or service you wish to appeal. Web 0:00 / 6:17 benefitscal: Web there are 2 ways that a party can request a redetermination: Send the form with proof by the due date of easy ways to give us your form and proof: Benefitscal 3.48k subscribers subscribe 112 share 19k views 1 year ago benefitscal help videos.
Redetermination Form Ywca 20202021 Fill and Sign Printable
This is called an annual redetermination. Specific service (s) and/or item (s) for which a redetermination is being requested. Case number social security number (optional) print your full name birth date (optional) (mm/dd/yyyy) current street address, apartment number city/state zip code mailing address city/state zip code Filling out this pdf can be carried out with a smartphone or laptop. Date.
Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
Benefitscal 3.48k subscribers subscribe 112 share 19k views 1 year ago benefitscal help videos. Web there are 2 ways that a party can request a redetermination: Web a request for redetermination must be received within 120 days of the date of the initial claim determination. Web if you need help completing a redetermination form you receive in the mail, call.

Dpss Lacounty Gov Annual Redetermination Fill Online, Printable
Date the service or item was received (mm/dd/yyyy) item or service you wish to appeal. Health insurance premium payment program. If you’re sent a renewal form, submit your information by mail, phone, in person, or online, so you don’t lose your coverage. Web fill out and turn in the enclosed annual redetermination form. Filling out this pdf can be carried.

Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
Filling out this pdf can be carried out with a smartphone or laptop. Respond to the appointment letter; Send the form with proof by the due date of easy ways to give us your form and proof: Date the service or item was received (mm/dd/yyyy) item or service you wish to appeal. Web you can help make the process a.

Medi Cal Redetermination Form ≡ Fill Out Printable PDF Forms Online
Date the service or item was received (mm/dd/yyyy) item or service you wish to appeal. This is called an annual redetermination. Web there are 2 ways that a party can request a redetermination: Specific date (s) of service. Complete and return the form;

Fill Free fillable Form MC210 MEDICAL ANNUAL REDETERMINATION FORM
Formspal offers a simple and safe method to work with medi cal redetermination form. Specific service (s) and/or item (s) for which a redetermination is being requested. Responding to the appointment letter or the request to complete forms you have 30 days to: Health insurance premium payment program. Date of the initial determination notice (mm/dd/yyyy) (please include a copy of.
Form Mc 210 Rv MediCal Annual Redetermination Form (Farsi) printable
Web here’s how it works: Date the service or item was received (mm/dd/yyyy) item or service you wish to appeal. Begin editing current pdf form by just pressing the orange button beneath. Responding to the appointment letter or the request to complete forms you have 30 days to: Health insurance premium program (hipp) application.
Medi Cal Redetermination Form ≡ Fill Out Printable PDF Forms Online
Web the following tips will help you fill out medi cal redetermination form easily and quickly: By mail in the envelope that came with this letter. If you have any questions or need help filling out this form, call your worker at the telephone number listed on the annual redetermination notice. Return the form along with any. Filling out this.

Fill Free fillable Form MC210 MEDICAL ANNUAL REDETERMINATION FORM
Web if you need help completing a redetermination form you receive in the mail, call us or visit your local social security office. Health insurance premium program (hipp) application. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to appeal date the service or item was received.
Form MC210 RV NOTICE Download Printable PDF or Fill Online MediCal
Return the form along with any. Can help you complete this application during the interview if you did not fill out all sections or if you need to make changes. Web 0:00 / 6:17 benefitscal: Click the green arrow with the inscription next to move from one field to. Respond to the appointment letter;
Date The Service Or Item Was Received (Mm/Dd/Yyyy) Item Or Service You Wish To Appeal.
Specific service (s) and/or item (s) for which a redetermination is being requested. Beneficiary name medicare number specific service (s) and/or item (s) for which a redetermination is being requested specific date (s) of service You may need to complete a renewal form. Web here’s how it works:
Pdf Fill And Print Forms May Be Completed Online And Printed To Hardcopy To Be Signed And Mailed In Or Submitted In Person To An Eligibility Worker For Processing.
Web determination request form — 1st level of appeal. Formspal offers a simple and safe method to work with medi cal redetermination form. Benefitscal 3.48k subscribers subscribe 112 share 19k views 1 year ago benefitscal help videos. Web if you need help completing a redetermination form you receive in the mail, call us or visit your local social security office.
Filling Out This Pdf Can Be Carried Out With A Smartphone Or Laptop.
Web there are 2 ways that a party can request a redetermination: Beneficiary’s name (first, middle, last) medicare number. By mail in the envelope that came with this letter. Sign and date on the declaration and signature page î step 3.
Web A Request For Redetermination Must Be Received Within 120 Days Of The Date Of The Initial Claim Determination.
Responding to the appointment letter or the request to complete forms you have 30 days to: Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to appeal date the service or item was received (mm/dd/yyyy) date of the initial determination notice (mm/dd/yyyy) (please include a copy of the notice with this request) Respond to the appointment letter; Web fill out and turn in the enclosed annual redetermination form.